|
|
Caro Rodríguez
·
Mar 20, 2018
·
Berkeley, CA
· Joined Mar 2015
· Points: 25
I suffered a grade 3 ACL tear in my left knee two weekends ago skiing. I'm devastated –as would anyone who just found out the news. The doctor I'm seeing specializes in allograft (cadaver) ACL reconstruction and seems to suggest the below: - slightly shorter recovery time
- some risk of re-tearing in younger patients
- range of motion should feel as natural as prior to injury
- less painful than autograft
After reading a bit online, the majority of the forums I've read suggest that the autograft is the way to go in younger more active patients. I feel that I'm part of this category, but I also don't think that my activities are considered "cutty" –the one caveat here being that bouldering can be a bit unpredictable in how we land. I really don't want to risk tearing the graft after surgery. Below are the highlights for this type of graft: - longer surgery time/ recovery time
- more pain post-op
- kneeling can become an issue
- area where graft is taken from can be compromised
My longwinded note is to help phrase two questions: Which graft is right for me based on my activities? And are there any folks out there willing to tell me some inspiring recovery stories?? - I commute 10 miles roundtrip by bike everyday (pretty flat) –this is part of my daily sanity, I enjoy this ride so much.
- I climb almost everyday, mainly boulder, but will lead sport routes whenever I'm on trips
- I hike, bikepack, ski (although I'm not feeling particularly keen on returning to downhill for a loooong time)
Thanks, <3 Caro
|
|
|
dave rosen
·
Mar 20, 2018
·
Hershey
· Joined Oct 2010
· Points: 169
Have you brought up these points with your surgeon? He is far more qualified to make this call than anyone on an online forum.
|
|
|
Casey Erin
·
Mar 20, 2018
·
San Diego, CA
· Joined Jun 2009
· Points: 55
I tore my ACL and had it replaced with a graph from my patellar tendon, this was the preferred method as I was still pursuing NFL dreams. It stayed stable throughout my career but the graph site has always been an issue, my buddy had a graph from his hamstring and still feels it 10+ years later, nothing crazy - just notices "tightness". I would suggest getting more information on the cadaver ACL, hopefully you will be able to get some advice here about it. Some general advice I can give: listen to your doctor and therapist. Don't overdue it too early into recovery. I had a friend who was given the clear to top rope climb a few months after surgery, but no bouldering because of the blunt force from a ground fall. Well, he didn't listen, bouldered, and tore his new ACL. Also, try not to get too bummed about not being able to do much, you will be walking and biking fairly quickly into recovery. So you may not be running 5ks or skiing, but you will be able to get outside and hike and bike(with some restrictions).
|
|
|
Caro Rodríguez
·
Mar 20, 2018
·
Berkeley, CA
· Joined Mar 2015
· Points: 25
Thanks for the advice Russ. I'm 26 years old. Unfortunately, I'm not in LA anymore –in the Bay Area now. Know of any great surgeons out here? Otherwise, I'll still reach out to Kerlan. Russ Walling wrote:Which is best? No telling...... I lost both mine 25+ years ago and got neither fixed. Am I limited? Sure. Downhill with a pack is certain death. Good thing I don't do that... the only thing it really impacts me is getting a heel hook and then pulling with the heel. That no longer works. Never bothered me biking unless I was really pulling on the upstroke. Snowboarding was no problem. Landing big bouldering falls could be problematic. You are in the LA area... go the Kerlan Jobe out in west LA. Get the best recommendations you can, and make a decision from that. You did not say how old you were... generally I advise if you are young, get it fixed. If you are old, ride it out. I was kinda old at the time (like 30?) and decided to ride it out. And remember: pain is just weakness leaving the body. Get the most bomber fix you can. Kneeling is overrated, and they have pill for most everything these days. Good luck and hoping for the best recovery
|
|
|
Caro Rodríguez
·
Mar 20, 2018
·
Berkeley, CA
· Joined Mar 2015
· Points: 25
Thanks for the words of wisdom Casey. really means a ton. Casey Erin wrote:I tore my ACL and had it replaced with a graph from my patellar tendon, this was the preferred method as I was still pursuing NFL dreams. It stayed stable throughout my career but the graph site has always been an issue, my buddy had a graph from his hamstring and still feels it 10+ years later, nothing crazy - just notices "tightness". I would suggest getting more information on the cadaver ACL, hopefully you will be able to get some advice here about it. Some general advice I can give: listen to your doctor and therapist. Don't overdue it too early into recovery. I had a friend who was given the clear to top rope climb a few months after surgery, but no bouldering because of the blunt force from a ground fall. Well, he didn't listen, bouldered, and tore his new ACL. Also, try not to get too bummed about not being able to do much, you will be walking and biking fairly quickly into recovery. So you may not be running 5ks or skiing, but you will be able to get outside and hike and bike(with some restrictions).
|
|
|
Caro Rodríguez
·
Mar 20, 2018
·
Berkeley, CA
· Joined Mar 2015
· Points: 25
Not to the full extant that I've done here. The doctor seems to think that based on my activities a cadaver graft would be fine for me, but I don't think he fully understands the risks involved in bouldering. dave rosen wrote:Have you brought up these points with your surgeon? He is far more qualified to make this call than anyone on an online forum.
|
|
|
Tim Stich
·
Mar 20, 2018
·
Colorado Springs, Colorado
· Joined Jan 2001
· Points: 1,516
My friend is getting the patellar tendon graft this week at the Steadman Institute in Vail. My other friend never had hers repaired and I have never noticed any issues when we went climbing together. She told me recently that she had that injury, as I would not have guessed.
|
|
|
normajean
·
Mar 20, 2018
·
Reading, PA
· Joined Jun 2015
· Points: 110
caro toca roca wrote:I suffered a grade 3 ACL tear in my left knee two weekends ago skiing. I'm devastated –as would anyone who just found out the news. The doctor I'm seeing specializes in allograft (cadaver) ACL reconstruction and seems to suggest the below: - slightly shorter recovery time
- some risk of re-tearing in younger patients
- range of motion should feel as natural as prior to injury
- less painful than autograft
After reading a bit online, the majority of the forums I've read suggest that the autograft is the way to go in younger more active patients. I feel that I'm part of this category, but I also don't think that my activities are considered "cutty" –the one caveat here being that bouldering can be a bit unpredictable in how we land. I really don't want to risk tearing the graft after surgery. Below are the highlights for this type of graft: - longer surgery time/ recovery time
- more pain post-op
- kneeling can become an issue
- area where graft is taken from can be compromised
My longwinded note is to help phrase two questions: Which graft is right for me based on my activities? And are there any folks out there willing to tell me some inspiring recovery stories?? - I commute 10 miles roundtrip by bike everyday (pretty flat) –this is part of my daily sanity, I enjoy this ride so much.
- I climb almost everyday, mainly boulder, but will lead sport routes whenever I'm on trips
- I hike, bikepack, ski (although I'm not feeling particularly keen on returning to downhill for a loooong time)
Thanks, <3 Caro Caro, Sorry to hear about your injury. I ruptured my ACL in a downhill skiing accident three weeks ago and had an autograft repair last Thursday. I have known my surgeon for a while. He is excellent and I trust him. The info below is based on what he told me. He does not do allografts because he finds that about 30% of those patients have low grade continuous infections that do not go away. He thinks it’s due to other organs (heart, liver, corneas) being harvested before anyone gets to tendonts and therefore contamination. You are correct about the recovery being longer with the autograft. He said that the patella tendon where they take the graft from takes 9 month to fully heal. Which means no bouldering or other jumping sports until then because your knee’s ability to absorb the shock of landing is compromised. The new ACL, however, is as strong as the original in 3 months and he said stronger than the original in 6. I mountain bike, which might be a problem due to knees playing key shock absorbtion role, but you should be able to return to street biking much sooner. After the injury, I did two weeks of prehab PT to reduce swelling and increase ROM. Got the muscular control back and was starting to walk without crutches just before the surgery destroyed my new-found prowess. All I can say, the first week after surgery really stinks. Pain hasn’t really been a problem but mobility and self sufficiency are. You are in a thigh to ankle immobilizing brace including during sleep. I am also in CPM machine 4 hours a day but I don’t know if that’s universal. I am sure it gets better. You just have to remind yourself of that and keep doing the rehab. Good luck!
|
|
|
Michael Anderson24
·
Mar 21, 2018
·
Chattanooga, TN
· Joined Jun 2014
· Points: 45
Sorry to hear bad news! I tore mine ACL 4 years ago in a bouldering fall where I just landed wrong. I had an autograft repair done with my quadriceps tendon which is a little more rare. It healed to about ~95% of what it was originally. I could climb, heel hook, drop knee, etc all without pretty much any issue. 3 weeks ago I ended up taking another bad bouldering fall where I have possibility retore it (I have got differing opinions from a Doc and PT) and will be getting an MRI soon. Key take away points are as long as you rehab diligently you will bounce back relatively quickly and will be able to get back to climbing full strength. I found the mental aspect of the recovery pretty challenging once I was given the ok to climb again. But also since you said you a mainly a boulder, just keep in mind that no matter what graft type you choose, the repair will probably not stand up to a awkward/bad bouldering fall.
|
|
|
Caro Rodríguez
·
Mar 21, 2018
·
Berkeley, CA
· Joined Mar 2015
· Points: 25
Thank you so much for your thorough response T G. I've read it through a couple of times and would love to chat about this all more with you. I'll DM you. I'm particularly concerned with two things that I'd like to chat with you more about: - finding the right surgeon (for graft selection) and PT (for understanding my physical demands) –I don't want to compromise climbing AT ALL in the long run. I think I can live with a little pain in my knee if it means that I can work highballs without holding back for risk of falling.
- Also, I'm curious to know if there is any risk in waiting out surgery a bit. I'm realizing more from what I read online that strengthening before surgery is KEY. I've been biking and go to the gym everyday –will be focusing on leg specific exercises now. I'm hoping that during this time I'll be able to climb and do some of the things I love, but if surgery is the only way to get back to what I love, then I feel more inclined to get into surgery as soon as I can get my legs very strong to deal with post-op recovery.
Again, thanks so much for taking the time. T G wrote:I'm 20 years older than you, but I've been a lifelong competitive athlete: swimming, cycling (on and off road), snowboarder, climbing of all types. I tore my ACL in 2015 while skiing and had reconstructive surgery in early 2016. Here's what I can tell you from my experience, and from the mountains of literature I read before and after my own surgery. Please DM me if you'd like to talk over the phone- happy to do it. I talked to dozens of people before my surgery and during my recovery and I know it helped me a lot both in terms of deciding how to go about things and how to keep a good attitude about everything. - You're young and active. Ask more questions about graft type. Has your doctor asked you what your plans are and what kinds of things you want to do? That, combined with your age and current activity level should have a big impact on graft selection. The surgeon may also recommend a particular approach based on his/her skills and experience. Don't assume it's the best approach for you, but don't assume it's not the right approach, either. ACL reconstruction is done so often now that the prognosis for an excellent recovery is extremely high. I had a combination graft of auto-donated hamstring tissue supplemented with allograft (Peroneus longus to be exact). The hyperbole about post-op pain with an autograft was way overblown - at least for me. More on that below. I've read that auto-donated patellar tendon reconstruction can have more significant (and painful) recovery, but with a bomber graft- particularly for young, athletic folks. In the end my surgeon advocated for the combo graft with my own hamstring with the rationale that the auto-donated hamstring tissue would help my body incorporate the graft more naturally, and that the allograft tissue would supplement it both in terms of strength and integrity. It is true that allograft tissue can take longer to vascularize and incorporate into the joint, and there are a number of notable studies that seem to indicate that allograft tissue carries a higher risk of re-injury in young folks (younger than you). But don't overthink it too much- discuss it with your doctor, get a second or third opinion, and know that whatever choice you make you're likely making a good one. The reality is that barring complications the graft will be stronger than the original ACL...
- Looks like you're in the Bay Area. Depending on your insurance situation you might seek out a sports medicine facility if you haven't already and assuming your insurance would cover the facility. My situation was somewhat unique in that I tore my ACL almost at the end of the year, so I was able to select a surgeon and an insurance plan for the next year knowing in advance that I was going to have surgery. Because I've been a lifelong athlete, I wanted people advising me and working on me who have deep sports medicine experience and understand what it is to be an athlete. That went both for the surgery itself and for the PT afterwards. My surgeon had done primary research on ACL reconstructions and that was important to me.
- Work your ass off before your surgery to get strong in both of your legs, your trunk, and particularly your affected leg. I can't underscore this enough. In hindsight I was lucky in some ways that I couldn't schedule my surgery right away and I had 3 months to go to the gym every single day. I busted my butt with squats, lunges, step-ups and step-downs, leg presses, good mornings... you name it. And the entire time I rode my bike like crazy to maintain cardio fitness and to supplement the gym work. It's hugely, hugely important to go into your surgery as strong as you can be and to be motivated to continue the hard work afterwards. It pays off in recovery time and it's probably the single most important thing you can do that you have control over in this whole process. Before surgery it'll help you to get motivated and get strong. After surgery it'll help your mood and give you a sense of some control over your situation.
- Pain. I'd never had surgery before and post-op pain was my biggest fear. Everyone experiences pain differently-- so it may be different for you-- but for me the fear of pain turned out to be wasted energy. Medicine has gotten so good at pain management. Ask about a regional femoral nerve block-- they're magical. I had zero pain. None. Zip. Nada. For me the nerve block lasted about 36-40 hours post-op and I was off pain meds after 2.5 days. I didn't feel a thing immediately after surgery or at any time during my recovery...
- Pain from the autograft harvest site: Again, little to none. My hamstring was definitely pretty black and blue and a bit sore, but really nothing worse than a tissue tear. Not a big deal, at least for me.
- Everyone heals at about the same rate, so there's not much you can do to speed up your recovery. That said, I was way, way ahead of the curve in terms of the typical post-op recovery timeline. I had my first PT session three days after surgery. The 2nd week post-op I was on the exercise bike (six days after surgery). I'm 100% convinced this is because of all of the hard work I did before my surgery. Either way you're going to lose muscle mass really quickly due to edema and swelling in the joint, but the stronger you are going in the more you move things in your favor post-op.
- Buy or rent an ice machine. It may seem not worth it from where you're sitting now, but it was totally worth it. I used one of the cheaper DonJoy "ice bucket" type ice machines rather than the crazy expensive GameReady units. The ice machines let you keep the joint and surrounding tissue iced 24 hours a day for the first couple of days- which will help with swelling and pain management. I had a minor complication in that I iced too much and caused my skin to get irritated and the joint to react somewhat adversely (this was about two weeks post-op). But in general the ice machine is a must in my experience.
- Heed the advice you may get about being conservative in your return to activities. My surgeon was really vocal about warning me of the risks associated with starting to feel good around 8-10 weeks post-op. The irony is that about the time you start feeling really good again your knee will be the most at risk due to the way the body heals. Essentially the graft tissue starts to die and becomes the weakest it will ever be right around that timeframe. So you'll want to be extremely careful. That said- and again your mileage may vary- I had my surgery in late March and was climbing again by late June right around 12 weeks post-op. I was very, very, very careful. No risk of falling, no high stepping, no back stepping, no rushing up or down the trail to and from. Friends carried the heavy stuff in my pack. It took me almost 8 months to feel 'normal' again, and I was prepared for the first year post-op to be really conservative. Nonetheless I was able to be highly active, just in a different way. I was always mindful of not overdoing it and not doing things that put my healing knee at unnecessary risk.
- Your bike will become your best friend and your ticket to post-op freedom. If you like riding your bike you'll get to do a lot of it. Use it to your advantage.
- After surgery, do something every single day to help you with your recovery. If that means to rest, then rest. If that means to do some knee bends 2 days after surgery to get your joint moving-- do that. Do every little thing you can do, every day. Stay motivated, stay positive, and take it day by day. It's a long haul for sure, but just focus on every single day as it comes.
I'm now two years post-op and there's nothing I can't do. I still have a bit of scar tissue in the joint from the surgical tools banging around in there that occasionally gives me a bit of discomfort, but it doesn't keep me from doing anything and my understanding is that the scar tissue will break down over time. I still have to pay attention to muscle balance and do some extra work to keep my hip flexors and glutes super strong-- definitely more than I ever did before surgery-- but it's not difficult or an annoyance. Even now my affected leg is stronger than the unaffected leg (hence the muscular balance work I need to pay attention to- ironic!). So. Biggest thing I can reiterate is to do the hard work before your surgery and get in the frame of mind to continue that work after surgery. Think about it like you're training for a big event-- something you have to work at over the long term and stay motivated at. Take it day by day and you'll do awesome. It's a character building experience for sure.
|
|
|
Charles DuPont
·
Mar 21, 2018
·
Portland, ME
· Joined Oct 2017
· Points: 118
caro toca roca wrote:- Also, I'm curious to know if there is any risk in waiting out surgery a bit. I'm realizing more from what I read online that strengthening before surgery is KEY. I've been biking and go to the gym everyday –will be focusing on leg specific exercises now. I'm hoping that during this time I'll be able to climb and do some of the things I love, but if surgery is the only way to get back to what I love, then I feel more inclined to get into surgery as soon as I can get my legs very strong to deal with post-op recovery.
I tore my ACL 9 months ago and haven't yet had surgery. At the time I was climbing 4 days a week and mountain biking nearly as often. Right after it happened, I definitely took a 2-3 week break from doing anything physical out of discomfort, lack of flexibility and fear that I may make the matter worse. However, after those couple weeks and working on regaining full range of motion in the knee, I started top roping again and quickly got back to climbing and biking with the same intensity I was before the injury. 9 months later and thats still the case! I will say that I am definitely more conscious of how I fall when bouldering (always roll onto my back, never try to "stick" the landing) and am a weary of taking high impact lead falls. I took the year off of skiing however, and decided to get the surgery next month (patellar tendon graft) so I can hopefully be back to skiing next season. I would say that besides that, there hasn't been a massive difference in my active lifestyle since my injury so if you want to wait before the surgery, go for it.
|
|
|
d powledge
·
Mar 21, 2018
·
Montana
· Joined May 2009
· Points: 21
If you can, I would get a second or even third opinion for pure comparison. My wife tore her ACL a few years ago in a soccer game. One surgeon was pro cadaver, his physical exam was only focused on the knee ( and was about 30 seconds) and my wife was ready to get it fixed and scheduled the surgery. Second opinion surgeon, complete and thorough physical exam, said given her high level of activity he would avoid cadaver, and due to her flexibility/ROM/gait/muscle balance he advised avoiding the hamstring graft - so she went patellar tendon. Longer recovery and more painful? Hell yes. However, she has since met several others who are now on their second or third ACL repair after their original cadaver graft ruptured. So much variability though, graft vs patient vs surgical technique. Tough choice, but I'd focus on the long term and not the quick return to sport. Best of luck and keep your head up. Injuries just suck. http://jisakos.bmj.com/content/2/6/308 http://bjsm.bmj.com/content/44/12/833 http://www.nejm.org/doi/full/10.1056/NEJMoa0907797
|
|
|
Kevin Ross
·
Mar 21, 2018
·
San Francisco, CA
· Joined Sep 2014
· Points: 0
My wife had her ACL done a couple of years back. Her approach to surgery reminds me a lot of yours. She did incredible amounts of research and very heavily considered the consequences of each option. She was (is) also extremely active, and was very concerned about maintaining that post-surgery (bouldering, trad climbing, big wall climbing, snowboarding, splitboarding, biking, surfing, you name it). Her conclusion after doing her research was that she wanted a hamstring autograft (for the "pro" reasons you listed above). Surgeon was on board with that. Unfortunately, during surgery the surgeon found that her harvested hamstring was too small for the graft... so he ended up needing to do a cadaver graft after all. She was not happy. Fast forward a couple of years, and she is killing it. Sure, she would have preferred a hamstring graft, but it all worked out really well in the end (always conscious of it, but doesn't hold her back). (Nearly) as good as new! It's a long process, don't get me wrong, but there's a light at the end of the tunnel. My advice from watching her recover: get a continuous motion device post surgery and work on range of motion as soon as you can. Get an icing machine and ice that thing till the cows come home. Then do your PT religiously and (more importantly) DON'T overdo it - I have some close friends who overdid PT and have some pretty bad tendonitis. Since you asked for inspiring recovery stories, here's her rough timeline - I think it's pretty phenomenal (though sometimes it terrified me): surgery in mid to late January, intensive rehab for a few months (through May-ish), then we slowly got back into things. She was top-roping in the gym after only a couple of months, she was following multi-pitch trad by I believe late May (somewhere between 4-5 months post op), and we went on a full-on alpine climbing trip to the Bugs in July (yeah, that one was a little dumb). From there it was full steam ahead and she climbed the whole summer and fall, and snowboarded the whole winter. There's hope!
|
|
|
rgold
·
Mar 21, 2018
·
Poughkeepsie, NY
· Joined Feb 2008
· Points: 526
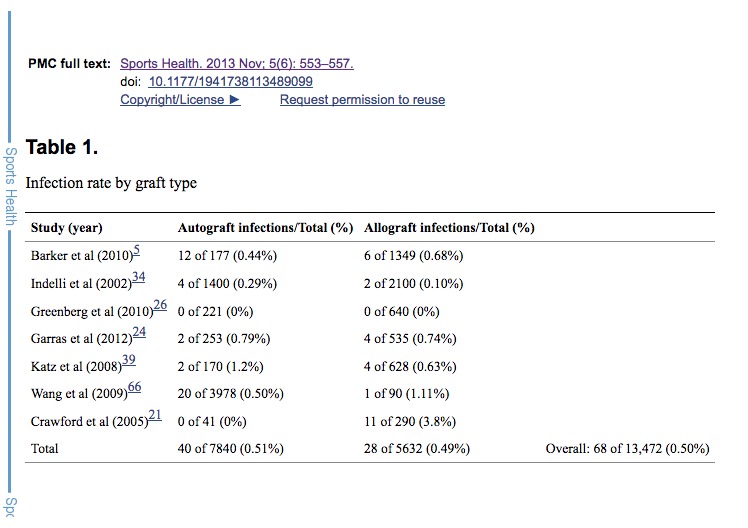
I tore my ACL six years ago, at 68 (so not terribly relevant to you). What might be relevant is that it was from a short jump-off bouldering. I considered myself sufficiently removed from being young to not take the youthful tendency for reinjury as a serious factor, and the easier recovery with an allograft, given that recovery periods tend to elongate as we age, was attractive. I don't ski or do other sports (any more) with significant twisting of the knee. I did some research at the time and didn't find anything remotely close to 30% patients with low-grade infections. If that was true, I doubt anyone would do the allograft surgery. For a reality check, here is a table from a 2015 issue of Sports Health (the specific reference is at the top). I went with the allograft. I had the repair done very soon after the injury, as my knee was very unstable and, unlike what others have reported, I couldn't see any path back to full activity. This means I couldn't do an preop physical training. Pain was not a significant post-op problem. I don't know if you have a significant other, but I did find I needed to sleep in a very spread-out position, and my wife and I used separate beds for a month or two before I could sleep comfortably in more normal configurations. I was back top-roping and doing relatively easy trad leading about 7 months post-op, but it was longer, at least a year, before I wasn't in some sense "aware" of my repaired knee. I did give up bouldering altogether, not so much because I considered the repaired knee vulnerable as because I just didn't want to go through that whole process again and at this stage of life am far more interested in moderate roped climbs anyway. Although I did professionally-supervised rehab for two or three months, I feel that one of the better things I did was to just go hiking. I started with short and gentle strolls, using walking poles (which I had never used before), and very gradually built up the length, strenuousness, and unevenness of the terrain. I got to liking the poles a lot and now use them not only for hiking but also for trail running.
|
|
|
Caro Rodríguez
·
Mar 22, 2018
·
Berkeley, CA
· Joined Mar 2015
· Points: 25
Thank you thank you Kevin for sharing. I am actually leaning more toward hamstring autograft after speaking to a couple climbers who underwent the surgery. A question to your wife about pre-op PT: did she use her brace during her exercises? I'm wondering if the brace lessens the effects of the PT. Kevin Ross wrote:My wife had her ACL done a couple of years back. Her approach to surgery reminds me a lot of yours. She did incredible amounts of research and very heavily considered the consequences of each option. She was (is) also extremely active, and was very concerned about maintaining that post-surgery (bouldering, trad climbing, big wall climbing, snowboarding, splitboarding, biking, surfing, you name it). Her conclusion after doing her research was that she wanted a hamstring autograft (for the "pro" reasons you listed above). Surgeon was on board with that. Unfortunately, during surgery the surgeon found that her harvested hamstring was too small for the graft... so he ended up needing to do a cadaver graft after all. She was not happy. Fast forward a couple of years, and she is killing it. Sure, she would have preferred a hamstring graft, but it all worked out really well in the end (always conscious of it, but doesn't hold her back). (Nearly) as good as new! It's a long process, don't get me wrong, but there's a light at the end of the tunnel. My advice from watching her recover: get a continuous motion device post surgery and work on range of motion as soon as you can. Get an icing machine and ice that thing till the cows come home. Then do your PT religiously and (more importantly) DON'T overdo it - I have some close friends who overdid PT and have some pretty bad tendonitis. Since you asked for inspiring recovery stories, here's her rough timeline - I think it's pretty phenomenal (though sometimes it terrified me): surgery in mid to late January, intensive rehab for a few months (through May-ish), then we slowly got back into things. She was top-roping in the gym after only a couple of months, she was following multi-pitch trad by I believe late May (somewhere between 4-5 months post op), and we went on a full-on alpine climbing trip to the Bugs in July (yeah, that one was a little dumb). From there it was full steam ahead and she climbed the whole summer and fall, and snowboarded the whole winter. There's hope!
|
|
|
Jon Nelson
 ·
Mar 22, 2018
·
Redmond, WA
· Joined Sep 2011
· Points: 8,611
·
Mar 22, 2018
·
Redmond, WA
· Joined Sep 2011
· Points: 8,611
normajean wrote:Caro, Sorry to hear about your injury. I ruptured my ACL in a downhill skiing accident three weeks ago and had an autograft repair last Thursday. I have known my surgeon for a while. He is excellent and I trust him. The info below is based on what he told me. He does not do allografts because he finds that about 30% of those patients have low grade continuous infections that do not go away. He thinks it’s due to other organs (heart, liver, corneas) being harvested before anyone gets to tendonts and therefore contamination. ... Thanks Normajean. That 30% seems huge compared to what I had heard before. Who is your surgeon and what is the nature of these low-grade infections? I am curious about this because I had an allograft in 2016, and ever since then seem to have much more joint stiffness in my lower back and hips. Perhaps it is all in the mind, but the thought came to me that perhaps something was introduced via the allograft. I've started checking it out with doctors, but am curious about what your surgeon found.
|
|
|
Kevin Ross
·
Mar 22, 2018
·
San Francisco, CA
· Joined Sep 2014
· Points: 0
caro toca roca wrote:Thank you thank you Kevin for sharing. I am actually leaning more toward hamstring autograft after speaking to a couple climbers who underwent the surgery. A question to your wife about pre-op PT: did she use her brace during her exercises? I'm wondering if the brace lessens the effects of the PT. No worries! Good luck to you! From my recollection she did not use the brace during PT, but did use it if she climbed.
|
|
|
Perry Norris
·
Mar 22, 2018
·
Truckee, CA
· Joined Nov 2014
· Points: 45
I tore my ACL skiing last year. I am 62 and my doctor told me try going without surgery and use a brace. I dialed back the skiing a bit, but otherwise don't really notice missing an ACL. I have friends who have similar stories. If I was in my 30s or 40s, I would however go with surgery.
|
|
|
rgold
·
Mar 23, 2018
·
Poughkeepsie, NY
· Joined Feb 2008
· Points: 526
I agree with TG. My knee was unstable and I felt the operation was essential, as I wanted to be able to navigate talus and scree, so it all depends. I certainly wouldn't take the fact that some folks manage without repair as any kind of gospel. You have to do what will work for you. My doc didn't use the motion or ice machines. I was walking on the leg (with a full-lenght brace) two or three days after surgery. The brace could be locked straight but I never had to do that. I did wear that brace for a week or two or three, don't recall how long. Later, I was fitted for a rigid brace that would not allow any lateral displacement of the knee joint. I hated it and stopped using it after a few hikes. I use neoprene sleeve brace with some mild lateral stiffening for trail-running.
|
|
|
normajean
·
Mar 23, 2018
·
Reading, PA
· Joined Jun 2015
· Points: 110
Jon Nelson wrote:Thanks Normajean. That 30% seems huge compared to what I had heard before. Who is your surgeon and what is the nature of these low-grade infections? I am curious about this because I had an allograft in 2016, and ever since then seem to have much more joint stiffness in my lower back and hips. Perhaps it is all in the mind, but the thought came to me that perhaps something was introduced via the allograft. I've started checking it out with doctors, but am curious about what your surgeon found. My surgeon (berkshiredocs.com/boa/drcanner.html) said that in 20-30% the contamination of cadaver tissue leads to chronic synovitis or accumulation of synovial fluid in the affected knee. I don’t think he meant other joints. Could it be that your back and hips are affected by your stance or gate which are still impacted? I would consult a good orthopedic specialist PT who does a lot of ACL rehab rather than surgeons.
|
|
|
Jon Nelson
·
Mar 23, 2018
·
Redmond, WA
· Joined Sep 2011
· Points: 8,611
normajean wrote:My surgeon (berkshiredocs.com/boa/drcanner.html) said that in 20-30% the contamination of cadaver tissue leads to chronic synovitis or accumulation of synovial fluid in the affected knee. I don’t think he meant other joints. Could it be that your back and hips are affected by your stance or gate which are still impacted? I would consult a good orthopedic specialist PT who does a lot of ACL rehab rather than surgeons. Thanks Normajean, I'll ask the doctor about this. I'll be seeing a physiatrist in a few weeks, which is a little like a PT but with more of a MD background.
|

 Continue with onX Maps
Continue with onX Maps Sign in with Facebook
Sign in with Facebook